New Lease on Life: Why Regenerative Medicine Is Finally Poised to Reach Its Potential
By Michael Blanding | Portraits by Danilo Agutoli

and green stains are for skeletal muscle-specific proteins MYOD1 and Myosin Heavy
Chain, respectively, and the nuclei are stained blue with DAPI. Image courtesy of Cellino.
Twenty-seven years ago, Doug Melton’s son Sam woke up sick and throwing up, and he and his wife rushed their six-month-old baby to the hospital. A doctor gave them a sober diagnosis: Sam had Type 1 diabetes, meaning his body was attacking the beta cells in his pancreas that produced insulin. Without regular injections, he wouldn’t survive. The pronouncement sent the family into turmoil. “You have a six-month-old son, and they can’t tell you, stop coming to me in the middle of the night and pricking me with that needle,” says Melton, then a Harvard biologist researching frog development. “They have to watch what they eat, measure their blood sugars, inject themselves with insulin. At what age do you give your child the responsibility to take that on, knowing that if they don’t, they will die?”
The next year, Melton completely changed his research practice to focus on finding a cure for the disease, a project that became more urgent when his daughter Emma also received a diagnosis at age 14. Now Co-Director of the Harvard Stem Cell Institute, Melton has placed his hopes on a bold proposition: using stem cells to regenerate the beta cells within the body to produce more insulin. Down the hall from Melton’s office, lab technicians inside a beta-cell “foundry” take stem cells — cells which have not yet differentiated into a specific tissue type — and subject them to a complex recipe of small molecules and growth factors. After some 15 different steps over six weeks, the solution resembles pink strawberry soda containing tiny snow-globe flakes, each cluster holding some 6,000 cells.
In 2015, Melton’s lab reported a breakthrough: the creation of the first functional beta cells, when injected into diabetic mice, allowed them to produce insulin for six months, demonstrating that a cure for the disease might be possible. “Now the question is can we figure out how to put it into humans?” Melton says. He created a company, Semma Therapeutics (named after this children Sam and Emma) to test that question, raising over $150 million in funding, with hopes to go into clinical trials within the next two years. The potential market for such a therapy is enormous. Currently, up to 40 million people worldwide suffer from type-1 diabetes, spending some $17 billion a year on insulin injections. In order to achieve success, however, Melton’s company will have to not only produce viable human beta cells, but also ensure they produce the right amount of insulin in the body, and protect the cells from being rejected by the patient they are trying to help.
Beta cells aren’t the only stem cell therapies that are currently showing promise. Other researchers — many in the Cambridge and Boston area — are using gene editing and other advanced techniques to turn stem cells into heart muscle and neurons that could regenerate damaged cells in the body. They have already used stem cells to effectively cure some rare diseases of the blood. Such regenerative therapies could produce new transplantable organs and even cure diseases incurable today. “I honestly believe this is achievable within our lifetime,” says Melton. “It’s not going to happen in a couple of years, but if we can combine genetic modification with the ability to make cells, it could change the practice of medicine.”

The Magic of Stem Cells
Stem cells have long been seen as a medicinal cure-all, unlocking the potential of the human body to heal itself. “In a way it’s the ultimate pharmaceutical,” says Bob Nelsen, Managing Director at ARCH Venture Partners, which has funded Semma and co-founded stem cell company Fate Therapeutics. “You can treat disease, or prevent disease, or reverse aging through the cells.” Despite the promise of so-called regenerative medicine, however, the reality has yet to live up to the hype. Beset by the controversy over embryonic stem cells, research into treatments lagged throughout the 1990s. Artificial organs created using stem cells simply fell apart. Biologists struggled to find ways to protect stem cells from being attacked by the hosts they were trying to heal, while timelines optimistically predicted a few years stretched into ten or more.
Recently, however, scientists and entrepreneurs have seen new hope for the field, as techniques have emerged to create stem cells without embryos. Since 2013, scientists have expedited cell transformation using gene editing technology CRISPR/Cas9, a technique to identify and replace specific snippets of DNA using guide-RNA, which functions like little zip codes to find the right place in the DNA strand to precisely change the genome. Along with that technology, new high-throughput screening techniques have allowed biologist to rapidly test multiple molecular compounds to transform stem cells. “We constantly try gaze into a crystal ball and understand what is going to be the next frontier in medicine,” says Jerel Davis, Managing Director of Versant Ventures, which helped found the company BlueRock Therapeutics. “A few years ago, we put regenerative medicine on our list as an inevitability, something that is going to fundamentally revolutionize how we develop therapeutics.”
In addition to the work in producing new cell therapies, Davis says, companies are developing new ways to mass-manufacture them, and regulators are becoming more open to approving them, putting science potentially on the cusp of a golden age of regenerative medicine. “Every cell type in the human body is a new platform for new therapeutics,” he says. While scientists have been making huge strides in creating new stem cells in petri dishes, however, the challenge now is to figure out how to get them into human bodies where they heal patients. “The part that hasn’t happened yet,” says Nelsen, “is to really understand how to deliver and target all of these cells in vivo.”
Despite the novelty of today’s stem cell therapies, scientists have known about the role of stem cells in animal embryo development for over 100 years. By the 1950s, biologists had begun exploring the role of two types of stem cells in human bone marrow: hematopoietic stem cells (HSCs), which create new blood cells; and mesenchymal stem cells (MSCs), which grow new fat, bone, and cartilage cells.
The first bone marrow transplant to treat patients suffering from blood cancers such as leukemia began in the late 1950s. For many years afterwards, however, bone marrow transplants have remained a treatment of last resort, since it requires killing patients’ existing immune system with intensive chemotherapy or radiation before transplanting new stem cells that can create healthy cells. Survival rates were only 60 percent when they first started, rising to 85 percent today, and even those who survive can experience complications including stunted development and infertility. “We brought people to the edge of death,” says David Scadden, Co-Director of the Harvard Stem Cell Institute, whose office is one floor down from Melton’s. “It was almost at the bounds of what was ethical. But when it worked it was miraculous.”
Like Melton, Scadden was motivated to study stem cells through a personal connection: the pain his mother underwent struggling with leukemia. He has currently spent much of his time in the lab focused on creating safer and better techniques for bone marrow transplants to treat cancer. Scadden is focusing on the HSC “niche,” the unique chemical environment within the blood marrow that allows stem cells to thrive. Based on the analysis of high-throughput chemical and genetic screens, his lab is trying to recreate that environment in a dish in order to make more stem cells that function better. “For a long time it was a debate in the field whether cells had their own internal logic and followed their own program,” Scadden says. “But that’s not true. We were able to show that they don’t govern themselves; they listen to the signals around them. If a neighborhood goes bad, it can corrupt a cell.”
Scadden is now examining ways to treat cancer cells — not by killing them, but by treating them as stem cells that have been stuck in their development. If doctors can “change the neighborhood” with drugs to alter the chemical makeup of a cell’s niche. “Maybe treating cancer isn’t about pounding it into oblivion with a hammer,” he says, “but by releasing the brake that has caused it to be stuck. Maybe a cancer cell is not a rogue cell, but a cell that has some normal features, but has been corrupted in its differentiation program in a way that has caused it to grow in an unregulated way.” By exposing them to the right environment of chemicals, maybe — just maybe — they can be reformed to become healthy contributors to the body. Through a company he co-founded named Magenta Therapeutics, he has been working to develop medicines.
Cellular Transformations
Other regenerative therapies have focused not on injecting stem cells into the body, but on transforming stem cells into other cell types to repair damaged cells within the body. In 1974, Rudolph Jaenisch and Beatrice Mintz succeeded in using a retrovirus to substitute a sequence of DNA in the nuclei of mouse stem cells in order to permanently alter their genome. This first “knock-in” mouse opened up new possibilities for stem cell therapies to overcome one of its primary challenges: the fact that new cells inserted into the body could be rejected by the immune system, leading to a serious complication known as graft-versus-host disease (GVHD). If stem cells could be created from a patient’s own DNA or cells, then the body would theoretically accept the cell as its own.
John Gurdon of the University of Cambridge in the UK had been able to show that DNA transfer into stem cells was possible decades earlier, by inserting the DNA into an embryonic stem cell, which successfully developed into a clone of an adult frog. By the 1998, scientists had isolated embryonic stem cells in humans (ESCs). At the time, however, controversy over the use of human embryonic stem cells threatened to halt regenerative medicine research, and Jaenisch and others began searching for a new way to create stem cells that would not involve using human embryos. Gurdon’s experiments had shown that any cell in the body had within it all of the genetic material necessary to create any other cell.
Photo by Doug Levy.
Enter Shinya Yamanaka and Kazutoshi Takahashi in the early 2000s. As researchers at Kyoto University in Japan, they identified just four active genes that could together make any cell pluripotent, essentially creating the equivalent of an embryonic stem cell from an adult cell. They created the first induced pluripotent stem cells (iPSCs) from both mice and humans in 2006. (Gurdon and Yamanaka shared the Nobel Prize for these discoveries in 2012.) That invention just over a decade ago opened the floodgates in regenerative medicine, showing that without any embryos at all scientists could create stem cells from a patient’s own blood or skin cells.
Jaensich, now at MIT’s Whitehead Institute, was the first to use iPSCs therapeutically in animals in 2007, when along with Tim Townes of the University of Alabama at Birmingham he was able to take cells from the tail of a mouse suffering from sickle-cell anemia, and induce them to become stem cells. The researchers then differentiated the cells into healthy HSCs without the sickle-cell mutation, and inserted them into the mouse’s bone marrow, creating new healthy red blood cells.
Researchers are now using all of these kinds of stem cells — HSCs, MSCs, ESCs, and iPSCs — to develop medicines for treating diseases in humans. Donald Kohn of UCLA, for example, has genetically modified patients’ own HSCs to treat adenosine deaminase-deficient severe combined immunodeficiency (ADA-SCID), also known as bubble-baby disease due to its severe inhibition of the immune system that can make a common cold fatal. Last year, he announced that nine out of ten children in clinical trials were cured from the disease.
Other clinical trials are currently underway to use patients’ own genetically modified HSCs to treat other blood disorders such as sickle-cell anemia and beta thalassemia in the same way — removing patients’ stem cells, genetically modifying them, and then returning them to the body where they will hopefully produce healthy red blood cells. Currently, three companies — Intellia Therapeutics, CRISPR Therapeutics, and Editas Medicine — are using CRISPR technology to edit the DNA in HSCs to attack diseases. The Switzerland- and Cambridge-based CRISPR Therapeutics began enrolling patients in a new clinical trial in October to remove HSCs of patients with sickle-cell anemia, genetically modify them to correct the mutation that prevents them from holding enough hemoglobin, and then insert them back into patients. It hopes to begin another trial targeting beta thalassemia in Europe by year’s end.
While CRISPR technology has advanced in editing genetic material, it can still be a challenge to get the guide-RNA into cells in order to make the necessary substitutions. Traditional genetic engineering using viruses is expensive and can potentially introduce unintended (and unwanted) genomic changes into cells; lipofection, which uses fat molecules to penetrate cell membranes, only works with certain cells; and nanoparticles can leave metal and polymer residues behind. To address that problem, Cambridge-based startup Cellino has developed a novel technique using laser pulses to get genetic material into cells. “It allows you to precisely manage the delivery of these zip codes into the cell at the right time in the right order,” says CEO Nabiha Saklayen.
The company grew out of the Harvard’s School of Engineering and the Wyss Institute, and is now financed and based at The Engine, built by MIT. Cellino’s technique uses a nanopattern surface studded with tiny pyramids covered in a metal coating. iPSC cells are cultured directly onto the surface, and a laser is pulsed across that same surface. As the laser energy is absorbed, it creates a nanobubble that temporarily opens a hole in the cell, allowing guide-RNA floating in solution to enter the cells. Within 20 to 30 seconds, the cell membrane closes with the material inside.
The technology can speed creation of cells over other techniques, Saklayen says. “One cell type that takes over 90 days in a dish, we’ve been able to create in three days,” she says. “It opens up a world of possibilities.” According to Chief Science Officer Stan Wang, formerly of Harvard Medical School, the company is planning to use a high-throughput system to rapidly experiment with engineering different cell types relevant to treating human disease as early as next year.
Beginning With The Blood
It’s no accident that the first stem-cell therapies involve diseases of the blood. Having single cells in a liquid medium makes it easier to take cells in and out of the body and still have them function. New research, however, has begun to concentrate on regenerating other types of cells and tissues. Cambridge-based BlueRock Therapeutics — funded by $225 million partnership between Versant and pharma giant Bayer AG — has focused on cells derived from ESCs and iPSCs, including dopaminergic cells to treat Parkinson’s disease and cardiomyocytes to repair muscle cells in the heart. “We wanted to create an off-the-shelf solution by identifying cell populations where we know what the deficiency is,” says Versant’s Davis. “In Parkinson’s, for example, we know you lose dopaminergic neurons and that leads to the symptoms, so BlueRock’s approach is to replace that exact cell type.”
To do that, the company plans to use a combination of transcription factors, proteins, and small molecules, in order to push the iPSCs down the path to becoming a specific cell type without directly editing their DNA. For dopaminergic cells, for example, it will use a protocol developed by Lorenz Studer, Director at the Center for Stem Cell Biology at Sloan-Kettering Memorial in New York and scientific co-founder of the company. The process uses a combination of three molecules to trigger something called the “wingless-type MMTV integration site (WNT) signaling pathway” to turn iSPCs into functioning nerve cells. These cells will then be implanted into the brain in an attempt to restore lost motor function.
For heart cells, the company plans on subjecting cells to a similar process in order to repair damaged tissue after a heart attack. For that process, the company is working with Michael Laflamme and Gordon Keller of the University of Toronto, which have managed to direct iPSC cells down the pathway into heart muscle cells. They are currently working on increasing the maturity of the cells in order to reduce their likelihood of arrhythmia (irregular heartbeat) before they are ready to implant into humans. BlueRock plans to enter clinical trials on the dopaminergic cells by year’s end, with cardiomyocytes to follow.

One company that is already involved in human clinical trials is ViaCyte, which like Melton’s Semma Therapeutics, is pursuing a stem cell–based therapy to tackle type-1 diabetes. The company has used small molecules to drive embryonic stem cells into something called pancreatic precursor cells, in the hopes that once implanted into the body, the cells will continue to evolve into endocrine cells that will produce insulin. “They are not functional at the time of transplantation, but they become so after development in vivo,” says ViaCyte’s Chief Science Officer Kevin D’Amour. Unlike in most diseases, in which researchers have to worry about the body rejecting implanted cells, the entire nature of type-1 diabetes is that the body attacks its own beta cells, whether they come from another donor or not.
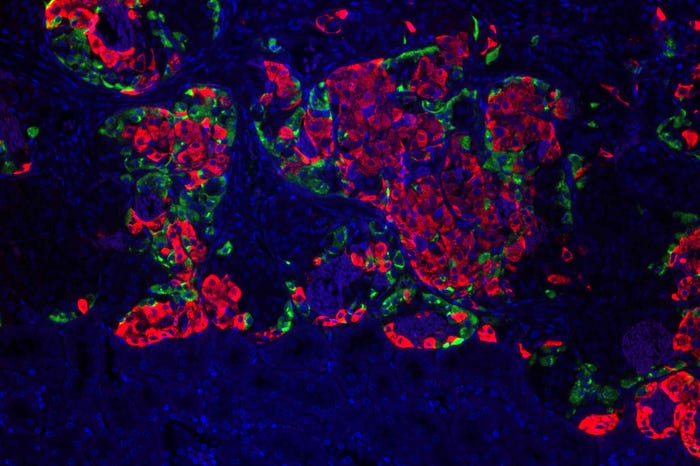
Image courtesy of Semma Therapeutics.
Because of that, ViaCyte has had to work to create a capsule in which to hold the implanted cells that will separate them from the body’s immune cells that seek to destroy it. Researchers often liken it to a “tea bag,” a semi-permeable membrane that can hold the cells and allow them to infuse the body without directly coming into contact with the blood. After implanting them in patients starting in 2015, however, researchers found that the body walled off the capsule with a layer of skin cells. “We saw a pretty aggressive response,” says ViaCyte CEO Paul Laikind. “The body is really trying to isolate that foreign body.” The company has suspended that trial while it works with W.L. Gore, the makers of Gore-Tex, to design a fabric for resisting the foreign-body response.
In the meantime, it started pursuing another clinical trial last year with a differently designed capsule that will allow blood vessels to penetrate the capsule and come into direct contact with the beta cells. While that should obviate the difficulties with rejection of the capsule, it will also require immunosuppression therapy to prevent the body from attacking the cells themselves. Even so, ViaCyte is hopeful that it can achieve therapeutic levels of insulin in the near term. “We hope it will be possible to demonstrate efficacy in six to twelve months,” says Laikind. Not taking anything for granted, the company has also partnered with gene-editing company CRISPR Therapeutics in order to try and genetically modify its precursor cells in order to protect them from the body’s immune response.
New Discoveries
While developments in stem cell biology from HSCs to embryonic stem cells to iPSCs has opened up new possibilities in regenerative medicine, one of the most exciting developments is the discovery that the body has multiple types of stem cells specific to organs, which may have the capacity to self-heal, if scientists can figure out how to switch them on. These so-called endogenous stem cells have been found, so far, in the liver, lungs, and intestine, and possibly the heart, and hold promise for regenerating their corresponding organs both inside and outside the body.
In 2009, Cedar-Sinai’s Eduardo Marban reported the results of the first clinical trial involving such endogenous stem cells, taking cells derived from the hearts of heart-attack patients, culturing them, and infusing them back into the body. The results, published in The Lancet in 2012, showed regeneration of healthy heart muscle, the first successful therapy of its kind. Despite such promise, however, patients did not see significant improvement in heart function, and later studies by Marban and others have shown mixed results.

Therapeutics and Magenta Therapeutics
A new direction in stem cell therapy is in treating endogenous stem cells while they are still inside the body, rather than removing them and re-inserting them. “The premise is that endogenous stem cells already exist inside the body, if we can only stimulate them to do what they would normally do,” says Derrick Rossi, a researcher at Children’s Hospital in Boston and co-founder of Intellia Therapeutics and Magenta Therapeutics. He recently became President and CEO of a new company, Cleveland-based Convelo Therapeutics, which is attempting to use endogenous stem cells in the central nervous system to treat multiple sclerosis. That disease is caused by destruction of the myelin sheath that wraps and insulates nerves inside the body, leading to a devastating range of symptoms from impaired vision to loss of muscle function.
Convelo is based on science by Case Western Reserve’s Paul Tesar and Drew Adams who discovered something called oligodendrocyte progenitor cells (OPCs) within the central nervous system, which could grow into cells responsible for re-myelination of nerves. They found that by targeting these OPCs with a combination of small molecules, they could block specific enzymes that inhibit their growth, and trigger them to regenerate myelin. With funding of $7.8 million from private donors, the company is now moving to test the drugs inside the body.
Tesar and Adams have not only used stem cells in their nerve cell therapy, but they have also used stem cells in the laboratory to construct human brain tissue on which to test their theories, rather than using mice or rats. Researchers have been using such “organoids” since 2008, when Yoshiki Sasai, a biologist at the Japanese research institute RIKEN, showed that embryonic stem cells could be coaxed into a dish to self-assemble into 3-dimensional tissue structures. Since then, scientists have produced organoids from both iPSCs and endogenous stem cells, creating virtual hearts, lungs, brains, kidneys, livers, and intestines. The development could reduce the cost and ethical concerns of using animals for research, as well as allowing researchers to experiment directly with human tissue, which might produce more accurate results earlier than using mice, rats, or monkeys. Scientists could even create patient-specific organoids that could allow them to personalize testing of potential treatments.
Growing tissues from such tiny organoids into full-fledged organs that might one day be transferred into the human body to replace a damaged or faulty organ, however, has proved a much more challenging endeavor. Back in the 1990s, Joseph Vacanti of Massachusetts General Hospital and Robert Langer of MIT pioneered a technique for building organs using biodegradable polymer scaffolding, seeded with stem cells. Build it, they thought, and the cells would do the rest, populating the scaffolding and performing the functions for which they were designed. While the process gave scientists key insights into how cells operate, it has ultimately been a failure.
Thus far, there has been few successful transplants of an artificial organ created through synthetic scaffold. In 2006, Anthony Atala of Wake Forest School of Medicine was able to grow artificial bladders and successfully transplant them into patients. He has since also used the techniques to construct artificial vaginas. In 2011, surgeon Paolo Macchiarini, at the Karolinska University implanted an artificial trachea into a cancer patient. Macchiarini repeated the procedure with a half-dozen other patients; however, nearly all of them died, and the university suspended its efforts after an inquiry questioning Macchiarini’s methods that found him guilty of ethical breaches in the way he represented the treatment.
All of these organs, however, are relatively simple in both structure and function. For more complex organs, no polymer scaffold was developed in the 1990s and early 2000s that was able to replicate their fine-tuned structure, especially the vasculature of millions of blood vessels needed to keep them healthy and alive. “At the time, there was no good scaffolding that could generate a human-scale organ,” says Harald Ott, a heart surgeon and organ engineer at Mass General. “The heart is not just a blob.” Attempts to regrow heart muscle by infusing stem cells into patients, however, also seemed not to be working. “It would have been great if it did,” Ott says, “but it’s not necessarily surprising that it wasn’t a magic bullet.”
Growing Organs
Starting in 2005, Ott began pursuing a novel approach to creating a new scaffold, by using donor organs, but stripping them of their original cells that might be rejected by a new host, while leaving the extracellular matrix intact. Then, theoretically, that scaffold could be repopulated with a patient’s own cells. Ott tried many different techniques and chemicals in an attempt to purge organs of their cells. “Up until the day it worked, everyone in the lab said, we can put you on our paper if yours doesn’t work out. It was a crazy high-risk project.” Finally, Ott hit paydirt with a combination of detergents including sodium-dodecyl sulfate (SDS), which caused cells to lyse, or break open, while keeping the extracellular matrix and its sturdy protein core intact.
The next problem was to put new cells onto that matrix. Ott started with a rat heart matrix, seeding it with fetal cardiomyocyte cells, which are already partially differentiated into heart muscle cells. After only eight days of maturation, the cells had grown enough so that they could be stimulated with an electrical pulse to produce a heartbeat. Ott’s lab has since used similar techniques using iPSCs to create hearts, kidneys, liver, and pancreases for rats and pigs, and has begun working on human organs. Recently, he created a rat intestine seeded with human stem cells that was able to absorb nutrients for four weeks, and a rat-sized pancreas that was able to cure diabetes for weeks. Despite those successes, he is realistic about how complicated a road he still has to travel. “It’s still very high-risk research,” says Ott, “It’s hard for me to get the financial support to perform this kind of academic research and development, and find the researchers who are willing to make this high-risk decision for their career.”
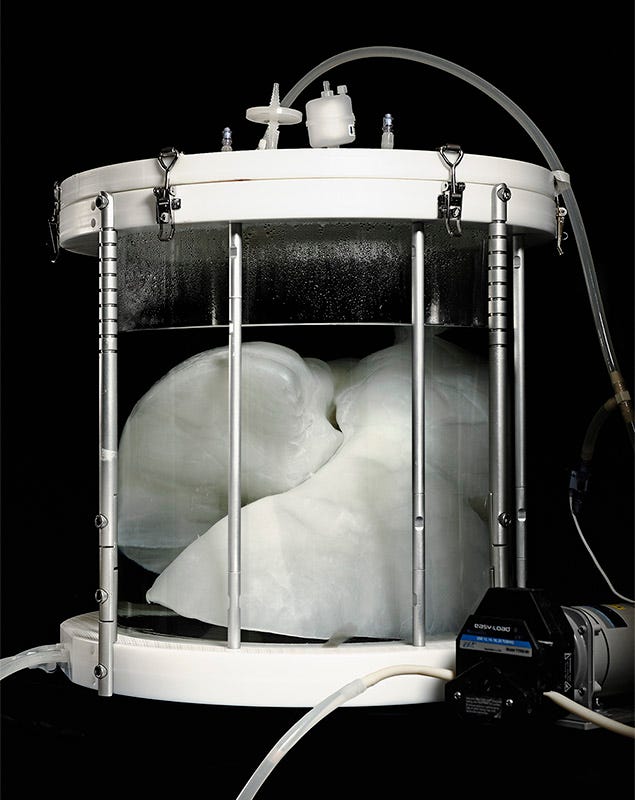
Image courtesy of The Ott Lab / Massachusetts General Hospital.
If scientists do succeed in creating organs artificially, however, it could dramatically improve the chances of survival for those needing organ transplants due to disease or injury. According to government statistics, last year some 35,000 organ transplants were performed in the U.S.; however more than 100,000 people are currently on the waiting list for an organ. Each day, 20 people die waiting for a transplant. Ott’s colleague at Mass General, Martin Yarmush, is working on ways to extend the lives of organs removed from the body so that more organs can survive to be transplanted. “There are millions of cadavers, from motorcycle accidents and such, that are perfect specimens of human beings, but after 30 minutes, an organ will lose all of its function,” says Yarmush, the Founding Director of the Center for Engineering in Medicine.
His lab has been working on techniques to perfuse organs that have been deprived of oxygen and nutrients, so they can be transplanted. So far, he has been able to take a rat liver that has been 60 minutes outside of the body at room temperature. “You put it into a perfusion device and perfuse it with media and other goodies, and you can get nearly 100 percent transplantation rate, if you leave it out for 60 minutes without putting it in a restore solution, you get zero.”
Another colleague at Mass General, Mehmet Toner, is working on ways to extend the life of organs for even longer periods of time. Even if an organ is kept cool, he says, it can’t be stored for more than a day outside the body. Freezing an organ down to cryogenic temperatures, however, damages vital tissue function. Toner’s lab is working on ways to preserve organs by cooling them down to intermediate temperatures, cool enough to slow metabolism long enough to preserve them for weeks or months without damaging them. Currently, he’s been able to preserve a rat liver for a week before transplanting with no harmful effects. It’s important to note that alternative organ preservation techniques using warm, flowing, nutrient-rich blood, like the Transmedics Organ Care System, represent a fundamental step forward from traditional cold ischemic storage, but do not address the longer preservation timelines being investigated by Toner’s lab.
Combined with techniques to create artificial organs, preservation technology like Toner’s could bring us closer to a day when organs are available “off-the-shelf” for patients, ready to be used at a moment’s notice — whether they are generated from their own cells or created from iPSCs. “When you need an aspirin, you don’t call someone who makes it for you, you go to CVS,” says Toner. “For cell therapies to become easily usable, you need to be able to stabilize them so they can be used when needed.”
Pig Hearts and Organ Printing
A more radical method to ensure we have viable organs available when we need them is being developed by George Church, a geneticist at Harvard Medical School and Harvard’s Wyss Institute for Biologically Inspired Engineering who helped invent CRISPR. Among other projects, he and former graduate student Luhan Yang are working to develop organs in pigs for transplanting into humans, a method known as xenotransplantation. Previously, he says, scientists have explored the idea of using pig organs as scaffolds, decellularizing them and replacing them with human stem cells. To Church and Yang, however, that just requires an extra step. “You are going to sacrifice the animal anyway. With the option we are pursuing, one animal can produce dozens of useable components for transplantation, and you can synchronize it before and after so they are ready when you need them,” he says.
Using pig organs poses its own challenges, however. One large concern is the presence of porcine endogenous retroviruses (PERVs) that could infect human cells and cause disease; the other worry is that the human body might reject the organ outright as a foreign object. Church and Yang formed a company, eGenesis, to tackle these issues. In 2015, they succeeded in using CRISPR to knock out the PERV genes in more than 60 different places in the genome of a pig; now, they are in the process of breeding a strain of PERV-free pigs in China. “We don’t have to do any fancy molecular biology; we can just breed them like pigs,” Church says. Now, the company is working on a separate project using CRISPR to knock out pig genes that provoke a response in the human immune system. “You trick the human immune system into believing that otherwise incompatible cells are okay,” Church says. Eventually, the hope is that they can breed the two strains of pigs together to produce pigs safe enough to donate their organs to humans in a virtually endless supply.
Both recellularization and xenotransplantation require some harvesting of organs in order to transplant them into a new body. A third method for organ engineering, however, aims to literally produce them from scratch. Church’s colleague at the Wyss Institute, Jennifer Lewis, has produced a 3D bioprinter that she is using to artificially print organs that could later be transplanted into humans. The idea grew out of earlier techniques to produce synthetic organs from polymers that could replicate human organs. In the midst of trying to create synthetic analogues for tissues and vascularization, however, Lewis and her colleagues decided to just create organs for real. “We said, we don’t have to emulate biology. We can do biology,” she says.
Wyss Professor of Biologically Inspired Engineering, Harvard John A. Paulson
School of Engineering and Applied Sciences.
Photo by Doug Levy.
Her technique consists of three different types of “inks” — a sacrificial ink that can help template vascular networks; a biopolymer ink to create a extracellular matrix for the organ scaffold; and finally, a cell-laden ink containing mesenchymal stem cells, iSPCs, or organoids to replicate the living cells of the organ. The machine would then coordinate all three of these inks to print the organ. “The challenge, of course, is to replicate the architectural complexity and cellular density of the organ,” Lewis says. “If you do all of that, then hopefully that means you have something that not only looks like an organ, but also functions like one.”
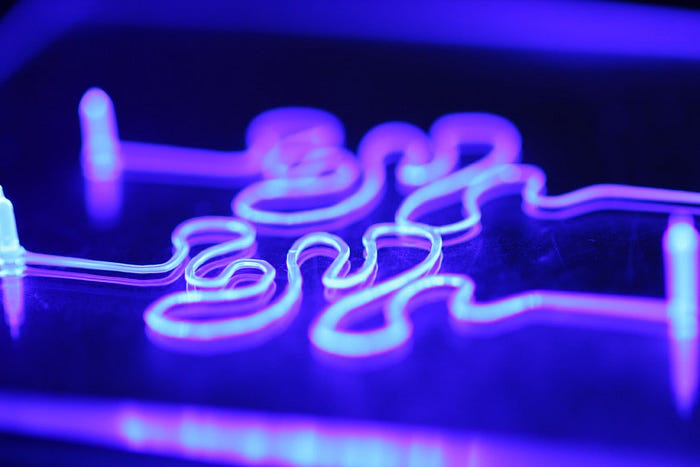
Image courtesy of Kimberly Homan, Jessica Herrmann, David Kolesky, and Jennifer Lewis from Harvard University and the Wyss Institute for Biologically Inspired Engineering.
Her next step is to print tissue that could be used in animals. “We are very much in the infancy in this process,” she admits, “but we certainly hope our work is providing some foundational basis for many labs around the world.”
Short of creating working organs for transplantation, 3D bioprinting can also produce artificial organ structures for medical research. So-called “organs on a chip” are like organoids in that they can consist of actual human tissue in vitro to test drugs and toxins as an alternative to animal testing. Using mechanical and electronic engineering, however, they can also be stimulated to recreate organ function as well. “We can mimic physiological breathing in the lungs, peristaltic-like motions in the intestine, and pulses in the heart,” says Don Ingber, the Wyss Institute’s Founding Director.
Ingber first participated in the creation of a lung on a chip, recreating alveoli sac and alveolic-capillary interface on a metal chip covered in silicone rubber. “It included incredible levels of functionality,” says Ingber. While traditional cell culture allows testing on a single cell type, organs-on-a-chip can include layers of different cells, printed on top of one another, to simulate the complete organ function. That in turn, could help drug companies more accurately conduct research into new therapies. “Seventy-five percent of drugs fail in clinical trials,” Ingber says. “That’s because animal models don’t adequately predict what will happen in humans.”
Ingber is scientific founder of Emulate, a company working to create a “body-on-a-chip” that would network several artificial organs together with channels to further explore the interactions between organs. In the future, those structures could be created with a patient’s own stem cells in order to test the efficacy and side effects of multiple drugs, before deciding on which to use inside the body. Outside of individualized treatment, a drug company could create an organ- or body-on-a-chip custom-designed for a certain genetic subgroup to demonstrate efficacy for a drug that might otherwise be seen as a failure in typical animal models. “That could be a game-changer for drug development,” Ingber says.
The future of regenerative medicine is likely to come not from any one technique, but from a combination multiple technologies: using CRISPR to edit genes and small molecules and growth factors to drive stem cells towards certain cell lineages, as well as using stem cells to build organs inside and outside of the body in order to improve human health. “In the early days of stem-cell biology, we thought it offered the opportunity to use things like blood stem cells as replacement parts,” says Scadden. While undoubtedly that is true, he says, “That’s a very narrow way of looking at regenerative medicine. Now it’s clear that they can also help us create models for diseases, and also give us medicine to trigger the cells inside of our body to heal itself.”
That combination of therapies, in turn, could fundamentally change the way medicine is practiced and life is lived. Patients could have individual therapies developed and tested for them on artificial organs outside the body before using them inside the body. And given the strides that regenerative medicine has made within the last 50 years, its likely that within the next 50 years what once seemed like science fiction could become a reality — a near-inexhaustible supply of replacement cells and organs available to us, created from our own cells or others, to repair and replace any part of the body that fails. If regenerative medicine is able to achieve that, as seems possible, it will truly be revolutionary.
